Chronic obstructive pulmonary disease (COPD) is a progressive disease that makes it hard to breathe. The commonest cause of COPD worldwide is cigarette smoking. Long–term exposure to other irritants, such as air pollution, chemical fumes or dust, may also contribute to COPD. Rarely, a genetic condition called Alpha-1 Antitrypsin deficiency causes COPD. People who have this condition have low levels of Alpha-1 Antitrypsin (AAT) — a protein made in the liver. Smokers with Alpha-1 Antitrypsin deficiency develop COPD at a young age. Although uncommon, asthma sufferers can develop COPD, especially if they are undiagnosed or untreated. To avoid this, it is advisable to consult a doctor for asthma to ensure the condition is well-managed.
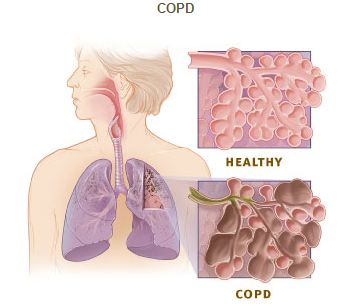
COPD includes two main conditions — emphysema and chronic bronchitis. In emphysema, the walls between many of the air sacs are damaged. This damage leads to fewer and larger air sacs instead of many tiny ones. As a result, the gas exchange in the lungs is reduced.
In chronic bronchitis, the inner lining of the airways is constantly irritated and inflamed. This causes the lining to thicken. Thick mucus forms in the airways, making it hard to breathe. Most people who have COPD have a combination of both emphysema and chronic bronchitis.
Symptoms
- Chronic cough
- Shortness of breath
- Wheezing
- Sputum production
- Chest tightness
- Ankle swelling (if severe)
Diagnosis
To confirm the diagnosis of COPD, a spirometry or lung function test (breathing test) is usually done. Other tests that may be done include chest X–ray, chest CT scan, and arterial blood gas. The bronchial challenge test (measurement of the sensitivity of the airways that is used to assist in the diagnosis of asthma) is usually negative.
Treatment
Quitting smoking is the most important step one can take to treat COPD. Success rates at quitting smoking are generally low (less than 10% success rate at six months). In such cases, most patients do need help, either in terms of pharmacotherapy or by attending smoking cessation clinics which may include one-to-one consultation with the provision of behavioural support in combination with nicotine replacement therapy.
Medications
While there is currently no cure for COPD, the progression of the disease can be reduced by early diagnosis and proper treatment management programmes. Patients who undergo COPD treatment will be able to better manage their symptoms and improve their quality of life. The usual treatment for COPD is the use of bronchodilators which are usually via the inhalation route. In severe cases, steroid inhalers are added to decrease the inflammatory response.
Flu Vaccine
Influenza (the flu) can cause serious problems for patients with underlying COPD. For such cases, the World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC, USA) recommends that patients with COPD get vaccinated against the flu at least annually.
Pneumococcal Vaccine
This vaccine lowers the risk of pneumococcal pneumonia and its complications. People who have COPD are at a higher risk of developing pneumonia than those who don’t. Professional societies also suggest that COPD patients be vaccinated routinely against pneumococcus.
Pulmonary Rehabilitation Programme
Pulmonary rehabilitation is a 6-week outpatient programme, with 3 times-a-week exercise plans designed for those with COPD. The programme includes aerobic and muscle strengthening exercises, disease and medication education, and nutritional and psychological counselling. The programme which equips the individual with skills to cope with daily activities, is usually delivered by a multidisciplinary team, including doctors, nurses, physical therapists, respiratory therapists, exercise specialists, and dieticians.
Long-Term Oxygen Therapy
Some patients with severe COPD have low blood oxygen levels. In such a situation, low–dose, continuous oxygen administered by a nasal cannula is usually prescribed. It may ease shortness of breath and improve quality of life. Two major studies also showed that such patients actually live longer than those not using oxygen.
Seek Treatment Early
COPD is one of the leading causes of disability and death. Due to the complexity of the disease, it is frequently misdiagnosed. Smokers or those who used to smoke are at higher risk of COPD. Exposure to air pollution, having a family history or respiratory conditions may also put you at risk. If your respiratory symptoms are not improving, it is important to see a doctor to prevent long-term lung damage and other life-threatening consequences.
